INTRODUCTION
Dental diagnostic X-rays are an essential part of dental practice. Although radiation doses have been reduced due to the development of digital techniques, dental diagnostic X-ray imaging remains one of the most common types of radiological procedures that are frequently performed in dental clinics for oral examinations [1,2]. Dental diagnostic X-rays for certain types of examinations, including bitewings, full-mouth series, and panoramic views, are in common use. Considering the lifetime frequency of exposure to dental diagnostic X-rays, even a slight increase in health risk would be of considerable public health importance [3].
Dental X-rays expose patients to relatively low radiation doses. However, the survivors of the Hiroshima atomic bombings provide evidence of increased cancer risk from low doses of radiation [4]. Repeated exposure could also increase cancer risk [5]. Exposure to dental X-rays is associated with potential risk of cancer, which was revealed in previous studies [6,7].
In the head and neck region, cancer risks caused by exposure to dental X-rays have been discussed. Although many epidemiological studies have reported on the association between exposure to dental X-rays and meningioma risk, it is still controversial, as some studies have shown a lack of association [8-10]. A meta-analysis study proposed that there is no clear evidence of a significant association between exposure to dental diagnostic X-rays and the risk of developing meningioma [11]. Several studies have found an association between dental X-ray exposure and increased risks of brain cancer [12,13], tumors of the parotid gland [14] and breast cancer [15] and thyroid cancer [16,17]. In particular, thyroid cancer is one of the most common cancers in the worldwide, and the side effects from dental radiation exposure are likely to contribute to its incidence due to the location of the thyroid gland. Repeated exposure to dental X-rays may result in various health problems including head and neck tumors and various systemic problems. Thus, we conducted a systematic review of papers that reported an association between dental X-ray exposure and overall health risks because no previous reports have summarized these associations.
MATERIALS AND METHODS
The patient, intervention, comparator, outcomes (PICO) method was followed as a viable tool for the systematic review process [18]. The PICO method for this systematic review was as follows. The “P” referred to all patients, the “I” referred to dental X-ray exposure, the “C” referred to dental X-ray non-exposure, and the “O” referred to brain cancer, meningioma, thyroid cancer, leukemia, and other cancers.
Search strategy and data sources
We searched the PUBMED, EMBASE, and MEDLINE databases and performed a manual search for papers. The databases were searched for all related paper published before December 2016. The paper published in all languages were selected. The following search terms were employed.
(i) PUBMED: (“radiography, dental” [MeSH Terms] OR (“radiography” [All Fields] AND “dental” [All Fields]) OR “dental radiography” [All Fields] OR “dental x ray” [All Fields]) AND exposure [All Fields] AND (“brain neoplasms” [MeSH Terms] OR (“brain” [All Fields] AND “neoplasms” [All Fields]) OR “brain neoplasms” [All Fields] OR (“brain” [All Fields] AND “cancer” [All Fields]) OR “brain cancer” [All Fields]); (ii) EMBASE: ‘dental’/exp OR dental AND (‘x ray’/exp OR ‘x ray’) AND (‘exposure’/exp OR exposure); (iii) Manual search was carried out using the reference lists of papers included in the systematic review, on review papers about overall health.
Study inclusion and exclusion
Two reviewers (S.Y.H, E.S.C.) independently assessed the eligibility of each study through the databases based on the predetermined selection criteria. Any disagreements were resolved through discussion. The inclusion criteria were as follows: (i) human study; (ii) health problems including cancers related to dental radiation exposure; (iii) the full text of the study was available. The exclusion criteria were as follows: (i) Radiation dose assessment study; (ii) Radiation safety management study; (iii) Review articles; (iv) Letter and recommendation.
Data extraction
Two authors (M.A.H. and H.Y.K) independently collected the following information: first author’s name, year of publication, study design, dental diagnostic X-ray type, health outcome, significance, risk estimates, and their confidence intervals (CIs). We tried to summarize the significance of test results according to the types of health outcomes and types of the dental x-ray. However, test results in some studies were expressed for more detailed categories such as age groups or frequencies of exposure and occurred either consistent which means that all test were significant or nonsignificant, or inconsistent which means that both coexisted. To solve the problem, the integrated significance was marked as having partial significance (PS) when only some of the characteristics were statistically significant, as having significance (S) when all the characteristics were significant, and as not having significance (NS) when all were nonsignificant.
Quality assessment
We assessed the methodological quality of each study using the Newcastle-Ottawa scale (NOS) [19] which uses a star rating system. A full score is 9 stars, and a score range 5 to 9 stars is considered to be a high methodological quality while a score range 0 to 4 is considered to be poor quality. Nineteen case-control studies and one cohort study were assessed on the quality excluding one case-report study.
RESULTS
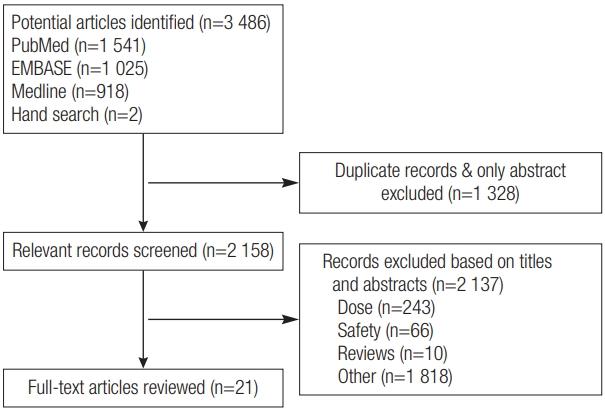
A total of 2 158 studies, except for duplicate studies, were initially collected. The abstracts and titles of the 2 158 papers were assessed. The full-text of the final 21 studies that were selected through classifications of exclusion criteria were read (Figure 1). We assessed information provided by the reporting of case–controls (n=19), cohort studies (n=1), and case studies (n=1). These studies were published between 1997 and 2015. These studies were conducted in the following countries: the United States (n=12), Sweden (n=4), Taiwan (n=1), Australia (n=1), Kuwait (n=1), Japan (n=1), and Syria (n=1).
Quality assessment
The quality of all included studies was summarized in Table 1. The median NOS score of the eligible studies was 4.0, 5.0, and 3.5 for meningioma and tumors in head and neck areas, thyroid cancer, and systemic health outcomes, respectively.
Health-related outcomes
Brain tumors
Table 2 shows 10 research papers on dental diagnostic X-rays and brain tumors. All were case–control studies. Five categorized or specified the types of dental diagnostic X-rays, while the other five did not. Two of these studies also included the panorama and bitewing types of examinations. Detailed analyses according to age groups or exposure frequencies were performed in five studies examining the correlation between the full-mouth examination type and brain tumors.
There were seven papers on meningiomas, three on gliomas, one on acoustic neuroma, and one on vestibular schwannoma, while two papers mentioned unspecific brain cancer. Seven papers reported a significant positive association and three presented a partially positive significant association, while eight had nonsignificant results. One paper reported a negative association between full-mouth X-ray exposure and glioma.
The association with meningioma was significant in 5 of 7 studies, while it was nonsignificant in the remaining 2 studies. Inconsistent results were reported on the association with glioma. A strong positive association was found in relation with vestibular schwannoma, while not with acoustic neuroma. The full-mouth examination type increased the risk of brain tumors significantly in three of the four studies.
Thyroid cancer
There were five research findings related to thyroid cancer (Table 3). As far as research design was concerned, four were case–control studies, while one was a cohort study. The five studies did not specify dental diagnostic X-ray types. In four of the five studies, there were significant correlations between dental diagnostic X-rays and thyroid cancer. One of these studies categorized the subjects by occupation and confirmed the correlation between dental practice and thyroid cancer.
Tumors in head and necks areas
Table 3 lists research findings on the tumors in head and necks areas. Tumors included laryngeal, parotid gland, and salivary gland cancers. As exposure to dental diagnostic X-rays increased, the risk of laryngeal cancer also increased. There was also a statistically significant correlation between full-mouth X-rays and salivary gland cancer, but not parotid gland cancer.
Systemic health outcomes
Leukemia and low birth weight have been reported as systemic health outcomes related to dental X-ray exposure (Table 3). One study categorized dental diagnostic X-ray types and examined correlations with low birth weight (LBW) and showed that only panoramic examination types had a statistically significant correlation with LBW. The risk of leukemia significantly increased in accordance with dental diagnostic X-ray exposure. A case report showed that thumb carcinoma occurred in radiographic technician who had performed dental diagnostic X-ray examinations for 15 years.
DISCUSSION
Patients are certainly exposed to dental diagnostic X-rays, and dental practitioners also potentially receive exposure. Although the level of exposure is lower than that of medical radiation, there is an innate risk from radiation exposure that cannot be ignored. However, there are a few studies on low-dose dental diagnostic X-ray exposure and health effects, except with respect to some parts of the body. In addition, papers report inconsistent statistical significances on dental diagnostic X-ray exposure and health effects, depending on the subjects and research design; therefore, related studies should be systematically organized. Hence, through a systematic literature review, this study included various studies with different research designs and examined the health risks associated with dental diagnostic X-ray exposure. For the literature review, this study examined twenty-one papers on dental diagnostic X-ray exposure and health effects.
Among twenty-one papers that reported a correlation between dental diagnostic X-rays and overall health, eighteen papers assessed a correlation with head and neck areas. The selected papers included ten on brain cancer, five on thyroid cancer, and three on head and neck areas other than the brain and thyroid. Since the oral cavity is anatomically located near the head and neck [36], dental X-ray examinations seem to affect the brain and neck areas. The correlation of X-rays with brain and thyroid cancers has been reported for many decades and seems to explain this finding.
Papers that reported a correlation between dental diagnostic X-ray exposure and overall health of dental practitioners were identified. The present study identified two papers on occupational groups [17,35]. According to a study on dental practitioners and thyroid cancer the risk of thyroid cancer was 13.1 times (95% CI 2.1–389) higher among female dentists and dental hygienists [17]. It is believed that women are more likely to have to thyroid cancer than men due to their hormones [37]. In a case report, a dental radiologist was exposed to dental diagnostic X-rays for 15 years and ended up developing finger cancer, which demonstrates that long-term exposure to low doses of dental diagnostic X-rays can pose a risk to health [35]. Another paper also reported that the cumulative dose for dentists who had worked for a long time was high [38]. Hence, dental practitioners should be aware of exposure to low doses of dental diagnostic X-rays, and risk of accumulative exposure to low-dose radiation from dental X-rays cannot be ruled out.
Dental diagnostic X-ray types were specifically categorized. Especially, panorama examination types are more commonly used than simple dental X-ray types, because panoramic diagnostic information coverage exceeds that of dental diagnostic X-rays [39]. Panoramic examinations also require fewer steps than conventional full-mouth examination types [40]. The full-mouth type had a statistical correlation with meningioma and salivary gland cancers. Meningioma cancer showed four times higher risk at younger ages (<20 years). Unlike adults, children are much more sensitive to radiation exposure due to active cell division [41]. In addition, the panorama examination type showed a correlation with meningioma cancer at higher exposure frequencies. Accordingly, a study on the amount of radiation exposure from each dental diagnostic X-ray type is needed. Nonetheless, the selected papers on thyroid cancer, which has a high level of radiation sensitivity [42], did not categorize dental diagnostic X-ray types, so this could not be examined.
There were some limitations of this study. This study did not specifically categorize exposure measurements, including exposure dose (mGy) and frequency, because each study has diverse radiation exposure categories. This study performed the only systematic review, not was extended to a meta-analysis, because the types of health outcomes were too diverse. However, we could identify trends in the dental diagnostic X-ray studies via this systematic literature review. This study has some important contributions. First, unlike existing literature reviews, this study covered diverse health outcomes as well as meningioma. Second, this study showed evidence that the increased risk of head and neck cancer due to exposure to low doses of dental diagnostic X-rays cannot be ignored.
It should also be noted that no studies have examined the specific types of dental X-rays and prevalence of thyroid cancer, which should be explored in further studies. Further studies are also needed to investigate the health effects of dental diagnostic X-rays in dental practitioners, who may be frequently exposed to high levels of radiation exposure.